If patients present with large stone burdens in both kidneys, bilateral PCNL surgeries can be performed at the same setting or alternatively staged at a later date as two separate surgeries. This decision will be made with you by your surgeon.
Home » pcnl
For kidney and ureteral stones that are too large (usually larger than 2 centimeters), too numerous, or too dense to be treated by extracorporeal shock wave lithotripsy (ESWL) or ureteroscopy, PCNL (percutaneous nephrolithotomy or stone extraction) offers a minimally invasive method of removing these stones.
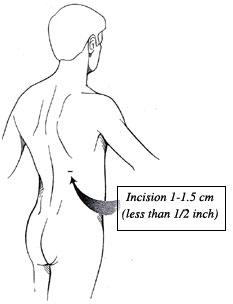
Historically, large kidney and ureteral stones were removed through open surgery, requiring a large flank incision. Percutaneous nephrolithotomy is performed through a 1-cm skin incision and thus minimizes incision size, pain, blood loss, blood transfusions and shortens hospitalization. This technique also has a higher success rate for clearing all stones in one setting than other techniques such as ESWL, which often require several procedures.
What to expect during you preoperative consultation
Prior to your initial consultation, it is important for patients to obtain all Xray films (e.g. KUB, CT scan, MRI, sonogram) and reports to bring to your surgeon for review. Your surgeon will review your medical history and perform a brief physical examination. A urinalysis will also be performed at your initial visit. All options for treatment of your stone(s) will be discussed at this time as well as the risks and benefits of each treatment. If your surgeon determines that you are a candidate for PCNL, you will then meet with a Surgery Scheduling Coordinator to arrange for the date of your operation.
Once your surgery date is secured by one of our Surgery Scheduling Coordinators, the items listed below will be ordered as necessary based upon your age, medical history and risk for surgery. These will be performed through a preoperative anesthesia consultation at the Presurgical Center at UF &Shands that will be arranged for you at your initial visit. During this consultation you will have the opportunity to speak to the anesthesia staff regarding the types of anesthesia available and the risks/benefits.
Medications to Avoid Prior to Surgery
The following is a list of medications to avoid at least 7-10 days prior to surgery. Many of these medications can alter platelet function or your body’s ability to clot and therefore may contribute to unwanted bleeding during surgery. Please contact your surgeon’s office if you are unsure about which medications to stop prior to surgery. Do not stop any medication without contacting the prescribing doctor to get their approval.
Aspirin, Motrin, Ibuprofen,, Vitamin E, Plavix
A formal list of these medications and others will be provided to you by our Surgery
It is very important that your urine remain free of infection prior to PCNL. Therefore if you suspect that you may have a urinary tract infection (burning on urination, blood in the urine, urinary frequency and urgency, fevers), please notify your surgeon immediate so that proper cultures and treatment may be provided.
PCNL is performed under general anesthesia with the patient lying face down on their abdomen. Once anesthesia is administered, your surgeon will perform cystoscopy (telescopic examination of your bladder) and instill xray dye or carbon dioxide into your kidney through a small catheter placed up through the ureter or drainage tube of the affected kidney to “map” the branches of the collecting system. This allows your surgeon to precisely locate the stone within the kidney and place a small needle through the skin under xray guidance to directly access the stone.
This needle tract is dilated to approximately 1-cm to allow placement of a plastic sheath and telescope to directly visualize the stone. Using an ultrasonic, mechanical or laser lithotripsy device, the stone is fragmented into small pieces and extracted out of the body through the sheath. On occasions, more than one tract may be required to access and attempts removal of all stones.
A small ureteral stent may be left draining the kidney to the bladder in addition to a nephrostomy tube draining the kidney to an external drainage bag at the end of the operation. The length of the surgery is generally 3-4 hours.
Potential Risks and Complications
As with any surgical procedure there are risks and potential complications that are associated with PCNL. Although rare, potential risks include:
During your hospitalization
Following your surgery you will be transferred to the recovery room and then to your hospital room once you are fully awake.
Although adverse events are rare following PCNL, it is important for patients to recognize these events and know when to contact their surgeon. You should contact your surgeon or primary care doctor immediately if any of the following occur:
What is the advantage of PCNL as compared to other stone treatments?
The primary advantage of PCNL over other treatments such as ESWL or ureteroscopy is that it provides a minimally invasive approach to treating and removing large stone burden in a single setting as compared to the need for multiple surgeries with the other therapies mentioned.
Whereas ESWL and ureteroscopy can be performed under intravenous sedation, PCNL requires a general anesthesia. Some patients may not be able to tolerate a general anesthesia due to their medical condition(s). As compared to other stone treatments, PCNL is slightly more invasive carrying with it a slightly higher risk. However, for most patients with large stone burdens, multiple stones or stones resistant to other forms of treatment, the benefits of PCNL outweigh the risks.
PCNL is an excellent option for patients with large kidney or ureteral stones (generally > 2 cm), multiple large stones, or stones resistant to prior treatment with ESWL or ureteroscopy.
Patients who have severe heart or lung conditions or have an uncorrectable bleeding propensity are not good candidates for PCNL. Patients with an active urinary infection are at a higher risk of sepsis during surgery and therefore should be treated with antibiotics to clear up the urinary infection prior to PCNL.
Multiple stones can be treated with PCNL. This is one of the advantages of this approach as a flexible telescope can be passed through the skin and directly into the kidney to attempt identification and removal of multiple stones in one setting. However, at times it may be difficult to visualize all areas of the collecting system despite the use of flexible telescopes and therefore some stones may not be retrievable. This may require placement of a second needle tract to access the remaining stones or a second PCNL procedure at a later date. Alternatively, PCNL can be used to remove the majority of the stone burden with ureteroscopy and ESWL left to clean up the remaining stone fragments.
Will I need placement of an indwelling ureteral stent following PCNL?
In most cases an indwelling ureteral stent is placed to promote drainage of urine from the kidney to the bladder.
The success of PCNL is dependent on many factors such as stone composition, stone size, number of stones, location within the urinary tract, patient body habitus (obesity), and anatomy of the collecting system of the kidney. Our surgeons carefully consider all of the aforementioned variables and will discuss this with you in order to maximize success and determine if PCNL is right for you. Overall stone free success rate is approximately 80-90% following an initial PCNL and 90-100% following a “second look” procedure.
Following PCNL, your surgeon will determine whether the treatment was successful based upon a CT scan that is performed during your hospitalization on the first postoperative day. If stone fragments remain within the urinary tract, more time may be required to allow for spontaneous passage, which often takes several weeks. Alternatively your surgeon may recommend further treatment with repeat PCNL, ESWL, or ureteroscopy.
Yes. Often due to stone density or size or difficult anatomy of the collecting system, fragments may at times remain in the urinary tract that may require a “second look” procedure to attempt removal. This is usually performed a few days after your initial surgery. Alternatively this second procedure may be staged at a later date depending upon your surgeon.
If patients present with large stone burdens in both kidneys, bilateral PCNL surgeries can be performed at the same setting or alternatively staged at a later date as two separate surgeries. This decision will be made with you by your surgeon.
Twitter feed is currently turned off. You may turn it on and set the API Keys and Tokens using Theme Options -> Social Options: Enable Twitter Feed.